
Introducing Structured Self-Research
A New Study Design for the Self-Experimenting Era

One of the biggest challenges in independent research is participant recruitment and adherence. When studies demand significant time, behavioral discipline, or unfamiliar protocols, participants need a good reason to stick through it.
All human research shares this problem, and the most common solution is motivating them through some combination of financial compensation and close oversight. But without institutional infrastructure, independent researchers can’t muscle through low compliance the way a pharma trial can. It is essential to make the participant experience as easy and valuable as possible in order to maximize participation.
This proposal describes a new study format designed to formalize the kind of personal experimentation people are already doing, with enough structure to generate real evidence, and low enough burden that thousands of people will be happy to participate.
There is a tradeoff in study design: the more methodologically rigorous study designs tend to be more burdensome for participants. But you don’t necessarily need maximum rigor to generate insight beyond what currently exists. We can use the Gold-Silver-Bronze framework to determine what level of rigor is appropriate for a given research context.
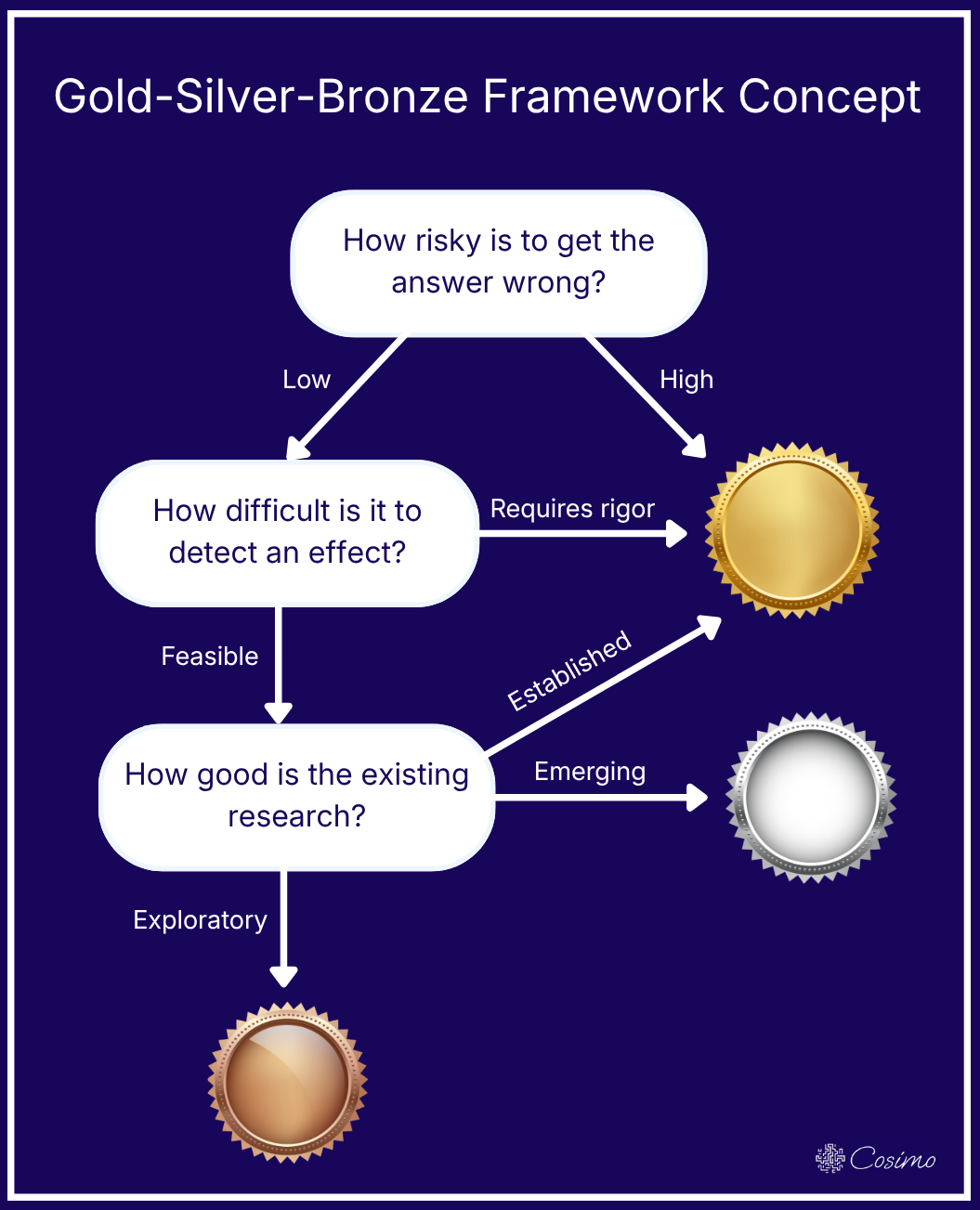
If a field is very established, any new contribution will require high methodological rigor. But if existing research is sparse, as it is for many supplements and other personal health interventions, almost any formalized study is an improvement over anecdotes. Additionally, if the question is relatively low risk and feasible to study, a silver- or bronze-tier approach may be entirely justified.
Every study format accepts some tradeoff between rigor and feasibility. We will briefly review the landscape of study formats, and then describe the structured self-research study, which fills an underserved space in the landscape.
Existing Study Formats
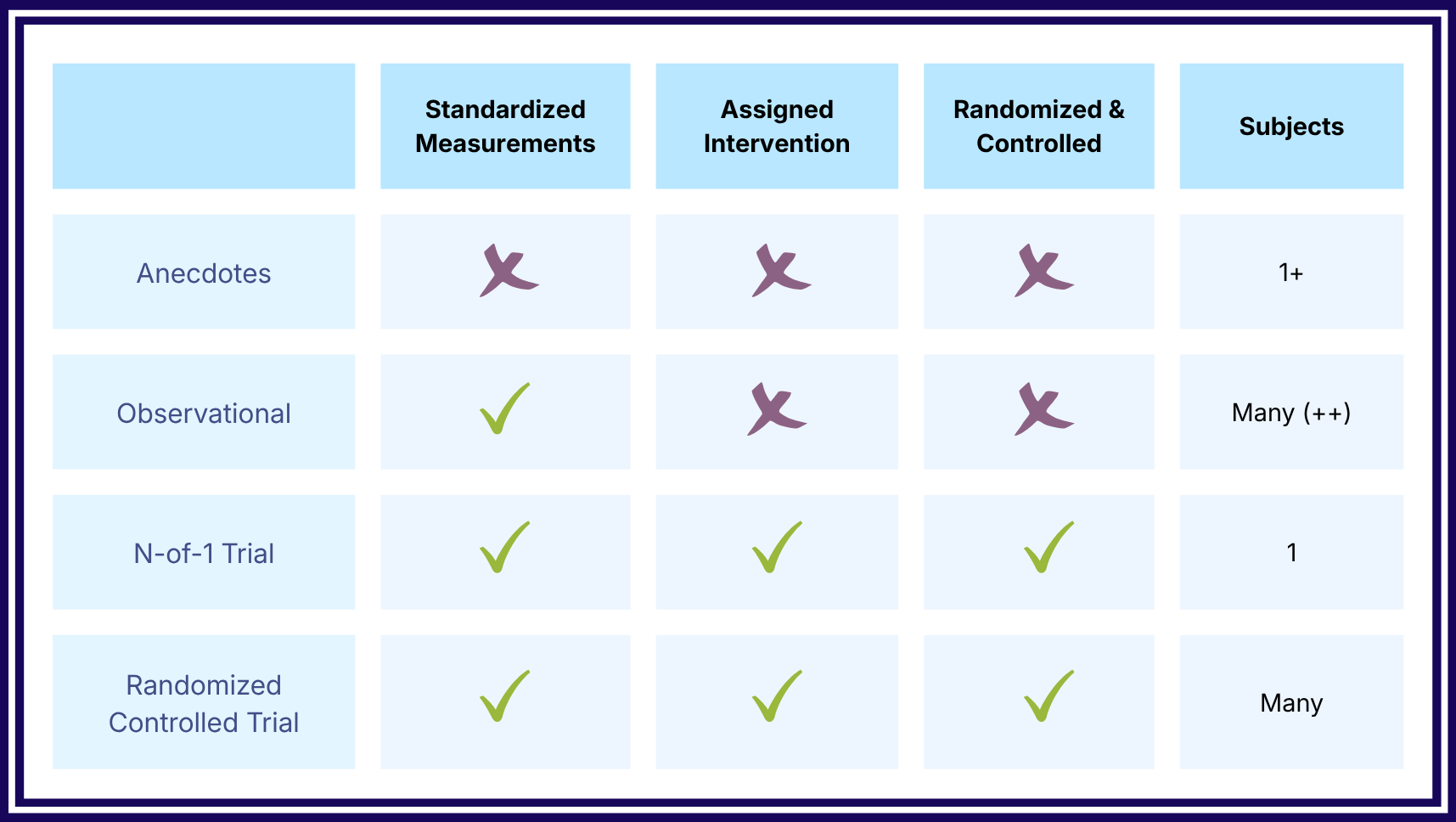
Anecdotes are individual reports of personal experience. Someone tries a supplement, notices they feel better or worse, and tells others. There is no structured measurement, no comparison group, and no protocol. Still, they can be informative in generating new theories, and they are especially useful between individuals with similar characteristics (e.g. a supplement that worked for your mother may work for you too).
Observational studies systematically measure what people are doing without assigning an intervention. These include cross-sectional studies, which involve collecting data on subjects at one point in time and looking for correlations, and cohort studies, which follow a group of people longitudinally and measure outcomes at multiple points. Within the latter you also have pre-post studies, where a group is measured before and after starting an intervention. All observational studies are subject to confounding, but the standardized measurements, statistical analysis, and multiple subjects add rigor beyond anecdotal evidence.
An n-of-1 trial is typically understood to be a controlled experiment with one participant, though the term is sometimes used more loosely as any single-person study. Done correctly, it produces strong causal evidence about how the intervention affects that specific individual: they serve as their own control across time, randomization protects against confounders, and blinding controls for expectation. However, the resulting evidence is not necessarily generalizable, and it usually requires greater discipline from the participant than an observational study.
The randomized controlled trial, often referred to as an RCT, is the gold standard of causal inference. A group of participants are randomly assigned to either receive the intervention or a control, and outcomes are compared between the groups. In a crossover trial, participants may receive either condition at different times. An RCT can be open-label, where everyone knows what they got, or double blind, where participants and researchers are both unaware of the conditions. They are expensive, operationally demanding, and unmatched in their ability to reveal causality.
Each of these study formats observes some tradeoff between participant ease and causal strength. Anecdotes are easy to generate and difficult to draw conclusions about. Randomized controlled trials require substantial commitment from participants and provide the strongest evidence for causal claims.
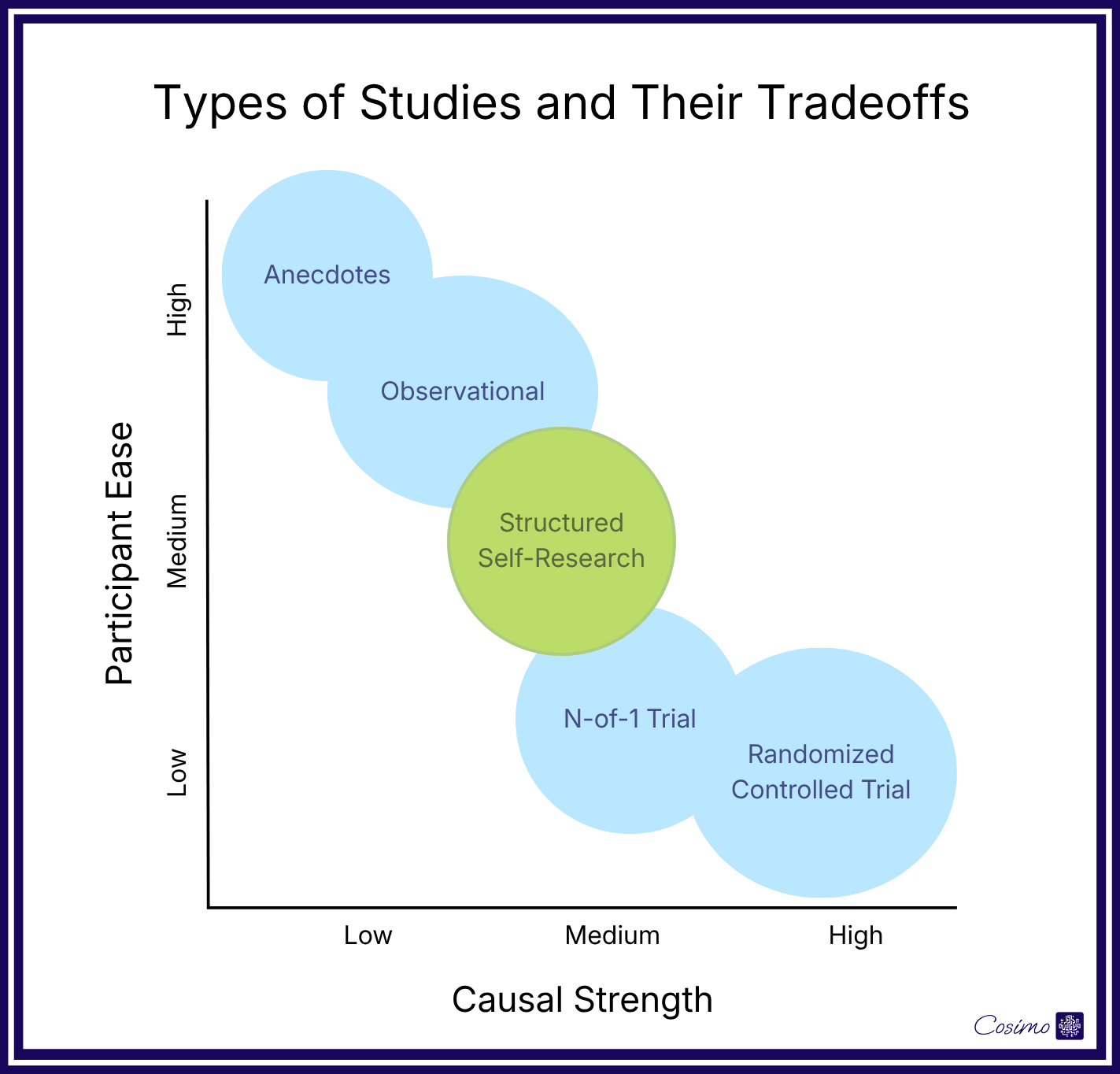
Introducing: Structured Self-Research
Structured self-research sits between extremes, balancing causal strength with participant ease. Participants follow a defined protocol, but they have agency in selecting which intervention to test and which outcome matters most to them. The study format has three key features designed to make it easy for individuals to formalize their own self-experimentation.
1. The protocol mirrors natural self-experimentation.
Like a pre-post observational study, the structured self-research study has three sequential phases (baseline, intervention, post) without randomization or blinding. This is close to how people often naturally try a new product or intervention — start in a state they want to change, introduce the intervention, compare how they feel, and sometimes check whether the effect persists after stopping. This structure formalizes what people already do.
2. In data collection, participant ease is the priority.
A daily check-in takes 15 seconds or less, delivered via a push notification at the same time every day. The reminder system is optimized for consistency and offers features like adaptive scheduling, customizable medium, and grace windows. Data collection is designed to be extremely low-cost for the participant.
3. The measurement targets what participants care about.
Often, this is a subjective measure. For example, we may directly track subjective energy, rather than measuring HRV or deep sleep duration, which are more objective and precise, but may be less personally meaningful. For each intervention, participants choose from a selected set of relevant outcomes. A participant testing a supplement for energy may be asked to rate themselves daily on three items (”energetic,” “sharp,” “motivated”) which are averaged to reduce noise. More precise measurements like wearable data or bloodwork are optional.
Structured self-research shares some commonalities with participant-led research, described by the Quantified Self community as “a collaborative form of investigation in which researchers and participants are the same individuals.”1 Structured self-research also involves increased participant agency, but it is more guided, with protocols and tools provided by scientists. It is also related to riff trials, where participants make their own modifications to an original protocol,2 but rather than exploring variations around the same intervention, structured self-research tests a set of standardized protocols across various participants.
Addressing Some Potential Concerns
How do you distinguish effects from placebo?
We accept that some portion of any observed effects could be due to expectation, and we report that alongside results. This study design is about quantifying what was previously just personal feeling, not completely isolating the cause of the change (as in observational studies, open-label RCTs, and other non-blinded research).
What about other confounders, like lifestyle changes that happen alongside starting a new supplement?
Individual differences such as genetics, baseline lifestyle, and personality, are the largest source of confounding in observational studies. In this phased study format, these are accounted for by each participant serving as their own control. Other factors that could change over the course of the study remain uncontrolled, but the phased format still offers an improvement over anecdotes.
Subjective outcome measures are unreliable.
They are indeed less precise than physiological measures, and often noisier. Subjective ratings can drift over time, vary with mood, and mean different things to different people. We try to reduce noise by averaging 3 measures and taking repeated measurements. Despite these limitations, they are often more aligned with what people wish to achieve with their health habits.
If everyone uses a different product, how do you know what’s actually being tested?
When participants source their own products, brand and formulation differences become part of the noise in the dataset. For studies where this matters most, we can either provide standardized products or recommend specific brands.
Are the people who would join representative?
Participants are self-selected, typically because they’re already interested in trying the intervention. This means that our results most accurately describe what happens to motivated self-experimenters, the same population who would benefit most from this evidence.
Example: A Structured Self-Research Study of BPC-157 for Pain Reduction
BPC-157 is not a “supplement” per se, but it’s the hot new biohack on the block, and it’s lacking solid evidence. Anecdotal reports of its effects on injury recovery and chronic pain are widespread on biohacker forums and podcasts, but published trials in humans are minimal.3
Users source it from gray-market peptide vendors, dose themselves based on internet protocols, and rely on personal impression to assess whether it’s working. This is exactly the situation for structured self-research: high participant motivation, no existing infrastructure for evidence generation, and people already experimenting in uncoordinated ways.
Population: Adults experiencing persistent musculoskeletal pain who are independently considering or already using BPC-157. Recruitment through biohacker and peptide-user communities.
Intervention: Participants self-source and self-administer BPC-157 according to a standardized protocol (dose, route, timing). Because the study is not providing the substance, the protocol specifies what participants should do if they choose to participate, rather than assigning treatment.
Phases:
Baseline (2 weeks): Daily check-ins establish each participant’s typical pain level and variability before any intervention.
Intervention (4 weeks): Participants begin BPC-157 according to the protocol. Daily check-ins continue.
Post (2 weeks): Participants stop the protocol but continue daily check-ins, allowing observation of whether effects persist or reverse.
Outcome measure: Subjective pain. Three short daily questions (“pain level right now,” “how much pain limited you today,” “how bothered you were by pain today”) averaged to reduce daily noise.
Participant Benefits: A personal report comparing their three phases, including average pain level, variability, and trajectory. Once the cohort is large enough, comparison to other participants with similar baseline pain levels and similar protocols.
Research Contributions: First-pass evidence on whether BPC-157 leads to subjective pain reduction with quantified, daily-resolution data.
Limitations: Participants self-select, source their own product, and are not blinded. The study cannot establish that BPC-157 caused observed changes, only whether changes were observed and how they were distributed across participants.
Conclusion
Structured self-research is not a replacement for randomized controlled trials. It occupies an underserved spot in the methodological landscape, using borrowed and well-understood methodologies and focusing on a worthwhile participant experience.
Structured self-research formalizes what people already do and provides tools to make it easier to generate quantified evidence.
If this resonates and you’d like to contribute to developing this methodology, please get in touch.
email: info@cosimoresearch.com
Grant, Azure and Gary Wolf. “Design and Implementation of Participant-Led Research in the Quantified Self Community.” Quantified Self. https://quantifiedself.com/white-paper-design-and-implementation-of-participant-led-research/.
There have been only three pilot human trials of BPC-157, with less than 16 patients each, in 2021, 2024, and 2025. All three studies are authored by Dr. Edwin Lee, a certified medical doctor and author of the book "The Fountain of Youth with Peptides." McGuire et al, 2025 provides a thorough review of the current evidence on BPC-157.